Dr. Ratnav Ratan offers suitable treatment options to resolve Metatarsus adductus in children
Metatarsus adductus in children is an abnormal gait developed in children on account of a foot deformity detected at birth. The child’s forefoot turns inwards and at times, it is diagnosed as a clubfoot condition. Hence, a careful clinical examination and an in-depth is a must for its accurate diagnosis. A pediatric orthopedic surgeon is called to assess the newborn’s feet if required.
Dr. Ratnav Ratan, Delhi’s leading pediatric orthopedic surgeon opines the above advice. He emphasizes that immediate treatment on diagnosis is crucial for such children.
Identifying Metatarsus adductus condition
Metatarsus adductus resembles intoeing or pigeon-toed in children. The child walks or runs with the forefoot turning inwards while there is a considerable gap between the toe thumb and the second toes accompanied by a high arch.
In medical terms, there is a medial deviation of the forefoot with regard to the hindfoot. The inward-turning can be flexible or inflexible. If the foot is flexible then correction by hand is possible to a certain degree. If the forefoot is inflexible then corrective treatment is inevitable.
Incidence of Metatarsus adductus
The incidence of Metatarsus adductus is one in a thousand births but does occur in families with past incidences of the same.
Causes of Metatarsus adductus
There is one reason for its occurrence which is the in utero crowding of the fetus during the pregnancy which leads to foot deformity and abnormal posture. Metatarsus adductus is associated with developmental hip dysplasia (DDH) and torticollis medical condition. If the child is detected with torticollis then there are 20% chances of the child developing developmental dysplasia of the hip –DDH.
These conditions are distinctly visible when the child is approximately 2 months old. It is also associated with breech deliveries, complicated deliveries while not ruling out chances of it occurring in a Cesarean delivery or uncomplicated vaginal delivery. If required, the doctor can further examine the child or recommend screening to accurately diagnose the condition.
The exact reason for its occurrence is still unknown. Also, it is more seen in the firstborn child.
Diagnosis of Metatarsus adductus
The treating pediatric orthopedic surgeon conducts a physical examination to diagnose this condition along with the child’s birth details and whether other family members have this condition. The doctor looks out for heel-bisector line and flexibility. There will be a distinct medial deviation of the forefoot on the hindfoot.
The doctor performs the passive manipulation procedure to test the flexibility score of the metatarsus adductus condition. The procedure involves pressurizing the heel gently to check its alignment with the heel. If the forefoot and the heel get aligned then the metatarsus adductus condition is flexible otherwise it is termed as non-flexible.
The pediatric orthopedic surgeon recommends x-rays if required.
Distinguishing between Metatarsus adductus and clubfoot (Talipes equinovarus)
In Metatarsus adductus condition, the forefoot turns inwards, i.e. the midline of the line. The affected foot is flexible at rest and passive abduction is also possible with sole stimulation. Metatarsus adductus condition is treated passively with promising results if treated early.
Clubfoot is diagnosed with the inward tilting of the heel i.e. from the midline of the leg and a medial deviation of the leg’s vertical axis i.e the adduction of the forefoot.
Children with Developmental dysplasia of the hip can also develop either metatarsus adductus condition or clubfoot deformity.
Treatment of Metatarsus adductus
Factors that determine the treatment of Metatarsus adductus
- Extent or severity of Metatarsus adductus
- Age of the child
- General health condition of the child
Generally, the foot straightens itself with the growth of the child.
The focus of the treatment is to align the position of the forefoot and the heel through the following treatment options –
If Metatarsus adductus is detected at birth, then the doctor will immediately begin treatment to correct the inward turning of the forefoot. There are very high chances that the forefoot will be aligned with the heel leading to the resolution of the deformity.
Observation for children with a flexible forefoot
Passive manipulation exercises and/or stretching – The treating surgeon or the therapist will teach the parents how to perform these exercises on the child’s foot.
Cast – If the metatarsus adductus condition does not improve, then long casts are used to stretch the soft tissue of the forefoot. The cast is changed every week or once in two weeks.
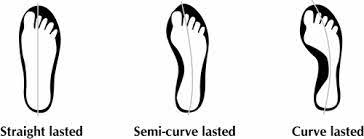
Straight last shoes – These specially designed shoes help to keep the forefoot in the correct position. These shoes do not have a curve in their bottom area.
Surgery – It is the last option to treat and correct a rigid or severe metatarsus adductus condition. The surgery helps to release the joints of the forefoot. Casts are also used after surgery to ensure the healing of the forefoot in the correct position.
The outcome of the treatment of metatarsus adductus
Passive manipulation is the most relied upon treatment with positive results if done at birth.
Also, correction with regular passive manipulation and/or stretching is attainable when the child reaches 3-5yrs of age. Surgical correction is advisable for residual deformities as suggested by the treating surgeon. Dr. Ratnav Ratan, a leading pediatric orthopedic surgeon in Delhi and Gurgaon recommends immediate treatment of metatarsus conditions as soon as they are detected to avoid corrective surgery during the growth years. Immediate treatment of metatarsus condition has promising results and relieves the children of pain and trauma associated with the condition and during the course of treatment.