Parents of infants and growing children can consult Dr. Ratnav Ratan, a consulting pediatric orthopedist in Gurgaon, Delhi NCR.
This helps rule out rickets or Blount’s disease as the cause behind the bowed legs condition in their child.
Bowlegs refer to a condition in which the legs of the patient are bent outwards, especially when the ankles are placed together.

Bowlegs cause outward bending of the legs and need careful orthopedic evaluation in growing children.
Bowling of legs is an incorrect alignment of the knees. It is also referred to as genu varum, tibia vara, bowed legs, or bowleg syndrome.
It is normal for an infant to have bowing of legs as they are folded when in the mother’s womb. The infant is likely to outgrow this condition when he or she starts to stand and walk, up to 2 years of age.
Usually, by the age of two or three years, the bending of the knees of the child begins towards each other, that is, inwards.
Parents should be concerned if they observe the following:
Along with the reasons mentioned above, parents should consult a pediatric orthopedic surgeon to prevent their child from developing bowleg conditions in the future.
The pediatric orthopedist will physically examine the child and suggest X-rays and EOS imaging in the standing alignment of the legs ranging from hip to ankle. This helps them understand the deformity with respect to location and extent.
Regular observation by the pediatric orthopedist is considered ideal in the initial stages of bowed legs.
Attempts will also be made to correct the angles of the leg through bracing.
Surgery is recommended as the last option. The pediatric orthopedist can recommend physical therapy to improve the bowed leg condition before or after corrective surgery.
The pediatric orthopedist may recommend a minimally invasive surgery to assist the guided growth process in the child. Through this surgery, the limb will be directed to grow in a linear direction.
In severe cases of bowed legs, osteotomy surgery is suggested. The surgeon performs an osteotomy on the upper shinbone to correct the alignment of the lower limb.
Braces work towards pulling the legs into a straighter position at a very gradual pace.
The infant or the child has to wear them till the legs are well straightened.
Bracing also helps in correcting the leg angles, but gradually.

Bracing gradually guides bowed legs into improved alignment over time.
This is a simple reversible procedure with minimal blood loss. The orthopedist arrests the growth of the growth plate present at the end of the long bone. This enables the other side of the growth plate to grow and gradually correct the bowed leg. This correction process takes nearly six to twelve months without using casts or braces.
Acute osteotomy involves a full correction of the bowed leg condition. The bone is cut and a plate with screws is inserted within to stabilize the cut bone. The entire correction procedure takes nearly six to eight weeks while the patient remains immobile during this period to ensure proper correction.
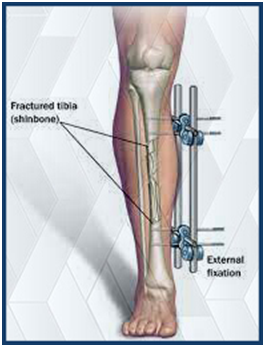
External fixators are adjustable frames used to gradually correct severe leg deformities.
Gradual correction of bowed legs using external fixators is recommended for children less than 10 years.
The orthopedic surgeon cuts the bone to apply an external yet adjustable frame to the bone using wires and pins. The frame can be adjusted as required.
Parents are trained on how to use and adjust the frame daily.
The child can perform daily activities normally without discomfort. Regular check-ups and follow-ups are necessary to monitor bone healing.
Blount’s disease is usually detected in obese children or children who begin to walk early. It is a type of bowleg deformity that happens at the knee joint or just below it.
The condition is identified by severe bowlegs and can affect either one leg or both legs.
It is necessary to detect Blount’s disease early as it helps in proper treatment and management of bowed legs. Patients can develop joint arthritis of the knee and degeneration of the lower limbs.
The two most important criteria for seeking surgical correction of Blount’s disease are:
The guided growth procedure is performed on children and teenagers. The pediatric orthopedist arrests the growth of the unaffected growth plate to enable the affected side of the growth plate to grow and catch up with the length of the normal growth plate. Small metal plates are used to prevent the healthy side from growing further.
This surgical procedure is performed if the patient has attained nearly or full growth and also in cases when guided growth has not delivered the desired results. The surgeon cuts the tibia bone just below the knee joint, realigns it correctly, and supports the bone using a plate or an external device on the leg till the corrected growth is achieved.