Is your child born with shoulder blades at different levels, where one shoulder blade appears higher than the other?
Does the neck look fuller on one side or is there visible restriction in shoulder movement?
Sprengel shoulder, also called Sprengel deformity, is a rare congenital skeletal abnormality involving abnormal development and elevation of the scapula.
Dr. Ratnav Ratan is an experienced pediatric orthopaedic doctor in Gurgaon, Delhi for diagnosis and treatment of Sprengel shoulder.
Sprengel shoulder or Sprengel deformity is an extremely rare congenital skeletal abnormality marked by an abnormally developed scapula positioned at a higher level than normal.
This condition develops during the early phase of fetal growth when the shoulder blade does not descend properly from the neck to its normal position.
The left shoulder is more commonly affected, although either shoulder or both shoulders may be involved. Sprengel deformity has also been observed more often in girls.
In children with this condition, the visible difference in shoulder level and contour is often the first sign noticed by parents.

Visible shoulder asymmetry in Sprengel shoulder deformity
Mild cases may go unnoticed until later childhood or adolescence, while more severe cases are visible much earlier because of the elevated shoulder blade and altered neck contour.
Early orthopaedic evaluation helps identify the degree of deformity and the effect on shoulder function.
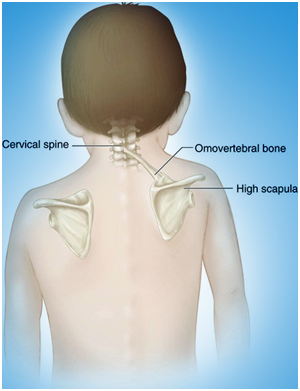
Scapular anatomy and abnormal elevated position in Sprengel deformity
The scapula, also known as the shoulder blade, is a triangular flat bone with nearly 17 muscles attached to it.
In Sprengel shoulder, the affected scapula lies closer to the body’s midline and is elevated by approximately 2 to 10 cm. The inferior pole rotates inward toward the spine, and the glenoid may also face inward.
Because of this abnormal position, the affected side of the neck often looks fuller and the shoulder contour appears uneven.
In medical terminology, Sprengel shoulder is also known as high scapula or congenital high scapula.
This condition may be associated with congenital scoliosis, fused ribs, cervical scoliosis, spina bifida, Klippel–Feil syndrome, and the presence of an omovertebral bone in the scapular region.
Identifying these associated conditions is important because they can influence treatment planning and long-term shoulder function.
The orthopaedic surgeon performs a thorough clinical evaluation while observing the characteristic signs of shoulder elevation, asymmetry, restricted movement, and neck contour changes.
The child may also undergo special X-rays and advanced imaging such as chest radiograph, CT scan, and MRI to assess the deformity in detail.
These imaging tests help detect the presence of an omovertebral bone and associated soft-tissue or skeletal structures, which is particularly important when surgery is being planned.

Dr. Ratnav Ratan, leading pediatric orthopedic doctor
Shoulders are almost at the same level, and the deformity is not noticeable when the child is wearing clothes.
The shoulders appear nearly level, but a visible lump of the elevated shoulder blade is present.
The deformity is visible, with a vertical difference of approximately 2 to 5 cm between the affected and unaffected shoulders.
The shoulder blade is very high, with its mid-angle resting near the back of the head, often accompanied by neck webbing and a short neck.
It is not possible to classify the severity in bilateral cases of Sprengel shoulder.
Treatment depends on the severity of deformity, cosmetic appearance, and the degree of restriction in shoulder function. The orthopaedic surgeon’s recommendation is the best guide for choosing the right management.
The main aims of surgery are to improve the cosmetic appearance and contour of the neck and to improve scapular function when it is significantly impaired.
The orthopaedic surgeon may release the tight attachments around the scapula, relocate the scapula to a lower position, and remove the omovertebral bone and related tissues if present.
The ideal age for this surgery is usually between 3 and 8 years, and many surgeons prefer correction before the child reaches eight years of age.
Surgery performed after this age, especially in adults, may carry a greater risk of unsatisfactory results and nerve injury because of tissue stretching and abnormal bone removal.
After surgery, the operated arm is usually placed in a sling for around three weeks.
This is followed by gentle range-of-motion exercises including both active and passive exercises, and later strengthening exercises.
Physical therapy may continue for up to six months to achieve the best functional and cosmetic outcomes.
Watch this case study video to understand the diagnosis, treatment planning, surgical correction, and recovery process for Sprengel shoulder.