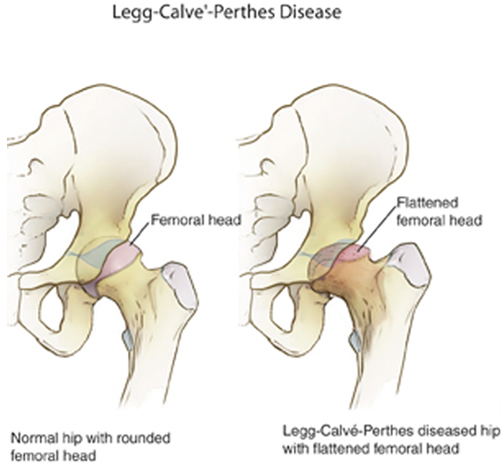
Legg-Calve-Perthes disease affects either one or both the child’s hips in the age group of 3 to 15 years. It is an uncommon disease and was identified by Arthur Legg, Jacques Calve, and Georg Perthes, independently following the arrival of X-ray imaging for diagnosing. It is also known as LCPD or Perthes. The loss of blood to the femoral head in the femur is the main reason for the Legg-Calve-Perthes disease.
How to identify a child with Perthes disease?
Keen observation of the child’s gait helps, especially when playing or during sports activities. Limping in the child or an abnormal running pattern does indicate issues in the hip or the hip joint. The child can also complain of pain in the hip, groin, thigh, and knee. The intensity of pain increases on activity while reducing on rest. The child also experiences painful spasms in the hip muscles on account of irritation. This painful condition may go on for a long period before the child gets evaluated medically for this condition.
Diagnosing the Perthes condition
The orthopedic surgeon will examine the child physically and seek the child’s medical history and x-rays to confirm the Perthes condition. The child’s range of motion and hip movement will be tested in-depth.
What happens in Perthes disease?
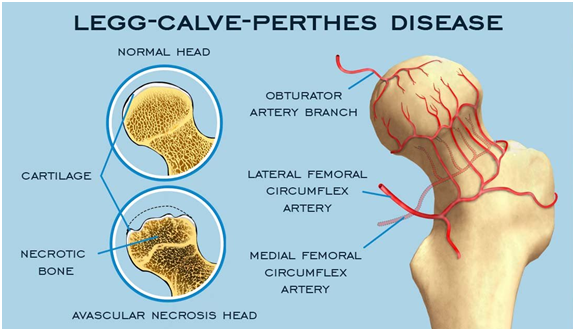
For unknown reasons, there is loss of blood supply to the femoral head, and a section of the bone of the femoral head dies. This dead bone is referred to as necrotic bone. The child or the patient is unaware of this loss as there are no symptoms experienced. After a couple of years of this loss, the body absorbs the dead bone and tries to regrow a new bone and repair the femoral head. This natural course and healing period of the body to resolve the loss of blood supply to the femoral head leads to the Legg-Calve-Perthes disease.
Yet another theory suggesting the loss of blood supply to the femoral head could be because of trauma that harms the blood vessels or form blood clots leading to the clogging of veins.
Another theory states repetitive mechanical trauma, delayed onset of skeletal maturity in the child or the child suffers from sickle cell anemia or hypothyroidism or epiphyseal dysplasia, Gaucher’s disease, bone graft reaction after bone marrow transplant, and leukemia.
There are negligible chances of the other femoral head getting affected with the Perthes disease in children with one affected hip.
Early treatment is essential as the child/patient, and the primary family is unaware of the onset of this condition and delay in its diagnosis. Also, children who have received early and suitable treatment of the Perthes disease can grow, live, and even play normally.
Treatment of Legg-Calve-Perthes disease
The orthopedic surgeon will conduct an in-depth evaluation and diagnosis of the hip condition depending upon the hip pain and stiffness in the child and the extent of the collapse of the head of the thighbone and then recommend the most suitable treatment.
The treatment of Legg-Calve-Perthes depends upon the following –
- The age of the child
- The range of motion in the hip
- The extent of Legg-Calve-Perthes disease in the child
Non-surgical treatments for Legg-Calve-Perthes disease
The orthopedic surgeon is likely to suggest
- Limited Activities
- Bed rest and traction
- Anti-inflammatory medicines
- Bracing or casting for the following purposes –
- To limit the activities of the joint movement
- To hold the head of the thighbone in the socket and
- To enable the thighbone to remold into the required round shape
How are bracing and/or casting useful in treating Legg-Calve-Perthes disease?
Tenontomy is yet another minor procedure performed to loosen the extremely tight adductor longus muscle in the groin, preventing the hip from rotating properly. The orthopedic surgeon inserts a very thin instrument into the muscle to loosen the muscle.
Use of A-frame as a conservative option to treat Perthes condition
To resolve the condition early non-surgically, the orthopedic surgeon will use Petrie casts, which are two long leg casts that help hold the legs apart using a bar. The legs so positioned resemble the alphabet ‘A’.
The orthopedic surgeon performs a tenotomy procedure, which involves cutting a tight tendon in the groin. Following this, an A-shaped frame – two casts held together by a bar helps keep the legs apart. An operating room is required to perform this procedure.
Also, arthrograms are special x-rays are taken to ascertain the degree of deformity and the likelihood of placing the femoral head in the right position. Hence, the procedure is performed in an operating room for taking arthrograms. A special dye is injected in small amounts into the hip joint to better view the femoral head during the procedure.
- Physical Therapy to make the affected hip muscles strong and to allow hip movement
Surgical treatment for Legg-Calve-Perthes disease
The orthopedic surgeon may recommend surgery to ensure that the head of the thighbone stays in the hip socket if non-surgical treatments have not yielded desired results. It is recommended to children with Legg-Calve-Perthes condition after they turn six years old. Also, if there is more than 50% damage to the femoral head, ensure proper bone growth for the required functionality.
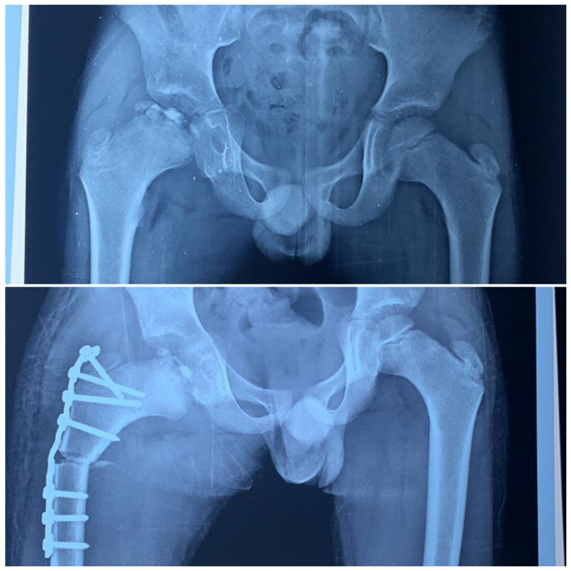
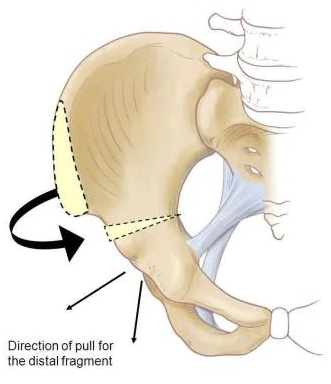
Femoral and Pelvic Osteotomy
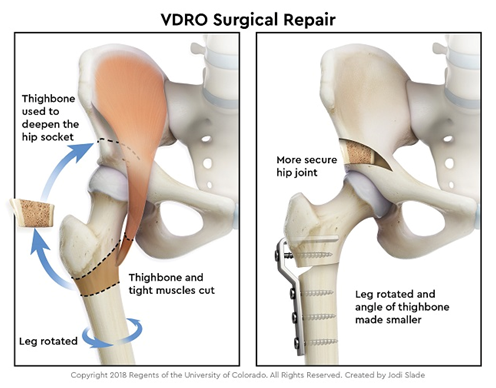
Femoral osteotomy is the surgical procedure in which the pediatric orthopedic surgeon works on the femur i.e. the thighbone and the socket, to accommodate the femoral head. If required, the femur is cut and adjusted to be well aligned, and the femoral head sits perfectly in the hip socket and is further secured with a metal plate and screws. The metal plate and screws are removed after the child has recovered from the disease.Along with femoral osteotomy the child may also need pelvic osteotomy or shelf procedure.
After fermoral osteotomy, the child has to wear a cast for many weeks to maintain the alignment. Once the cast is removed, physical therapy is required to regain muscle strength and range of motion. The child will have to use crutches or a walker to move around to reduce weight bearing on the affected hip.
If the Perthes condition is presented late i.e., after nine years of age, then the chances of conservative treatment and tested surgical procedures are less likely to have the desired impact. The focus is to attempt to change the shape of the femoral head or reduce the pressure in the hip joint. In addition, the orthopedic surgeon may opt for a combination of treatments to resolve this debilitating hip condition.
Hinge Abduction Condition in patients with Legg-Calve-Perthes disease
A patient with a hinge abduction condition will have pain and shortening. The patient will have an abnormal hip movement on account of avascular necrosis. The deformed femoral head is unable to slide within the acetabulum. Orthopedic surgeons recommend arthrodesis to resolve this condition.
Treatment of hip abduction condition involves an early transphyseal neck-head drilling, and protection with an abduction brace is advised at this stage. Also, prevention of the onset of Perthes disease in the opposite hip is possible with a transphyseal neck-head drilling, especially at the necrotic stage, when the disease has not exactly affected the joint.
Post the drilling procedure; revascularization begins from the surrounding area to the centre. While the surrounding areas of the necrotic zone also show healing, but it begins from the centre. The required reconstruction happens in less than one-third or half the time of the natural history of the disease.
The children with treated Legg-Calve-Perthes disease could develop hip issues later; hence, it is essential to go for regular orthopedic checkups until they become adults.