This is a case study of Untreated Developmental Dysplasia of hip (DDH) in a 6-year-old girl treated by Dr. Ratnav Ratan.
History
A 6-year-old girl had a left sided limp and shortening of left lower limb ever since she started walking. Her parents were uneducated and had run pillar to post for her treatment. No treatment was offered to her anywhere till that age. The child was otherwise healthy and had normal developmental milestones. Birth history was uneventful and there was no family history of similar illness. The child had normal IQ.
Examination
On clinical examination the child was active and playful. Higher mental functions were normal. No limb spasticity was present. She was found to walk with a short limb, abductor lurch to left side. The left hip could be seen translating proximally in the form of a mobile gluteal lump. The ipsilateral thigh and gluteal muscles were atrophied. Telescopy test was positive on the affected side with femoral head palpable superolaterally. The left femur was shortened by about 3 inches. Hip abduction was restricted to about 30 degrees. Adductor longus was extremely taut. Neuro-vascular examination was normal. The contralateral limb, spine & upper limb were normal on examination.

Investigation
X-ray and MRI examination of the hip were done. The femoral head was found to be dislocated superolaterally with a hypoplastic femoral capital epiphysis, increased femoral anteversion and extreme Coxa Valga and Acetabular dysplasia.


Diagnosis
The child was diagnosed to have Untreated/neglected Developmental Dysplasia of left hip (DDH).
Management
Open Reduction + Femoral de-rotation & shortening osteotomy + Salter Pelvic osteotomy.
Surgical Steps
Careful surgical planning was done to assess the degree of Coxa Valga, Anteversion & Acetabular Index. After thorough preoperative workup she was taken for surgery under General Anaesthesia.
An open reduction of the left hip was done through a bikini incision. The redundant hip capsule was opened up, hypertrophied ligamentum teres and fibrous tissue in the fossa were cleared. The hip couldn’t be pulled down to the socket.
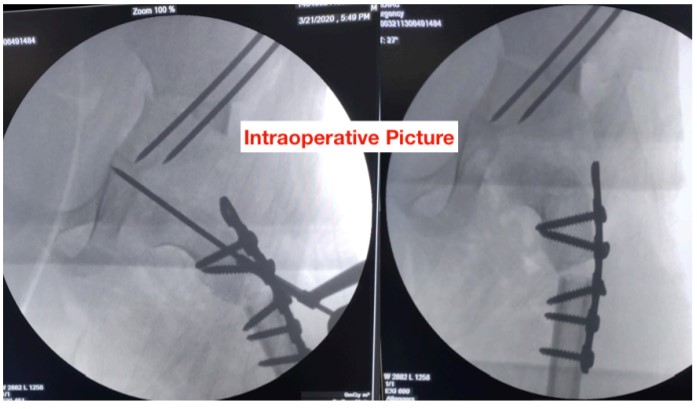
Proximal femur was osteotomised using a separate lateral incision. Hip was reduced and the amount of femoral overlap was assessed. 2.5cm femoral shortening and de-rotation was done and fixed with a plate. The hip was found to be stable after fixing the osteotomy. A temporary K wire was passed across left hip. Salter pelvic osteotomy was done using an osteotome to improve the acetabular coverage. Osteotomised femoral cortical ring graft was fashioned to fit the Salter osteotomy gap. It was fixed with 2K wires. After closure, a Hip Spica was applied.
Follow-up
At 6 weeks the spica was removed, K wires extracted. The hip was found to be stable. X-ray revealed good bony union of the femoral and pelvic osteotomy. The child was thereafter mobilised. She recovered her movements and muscle strength over next few months with extensive supervised rehabilitation.
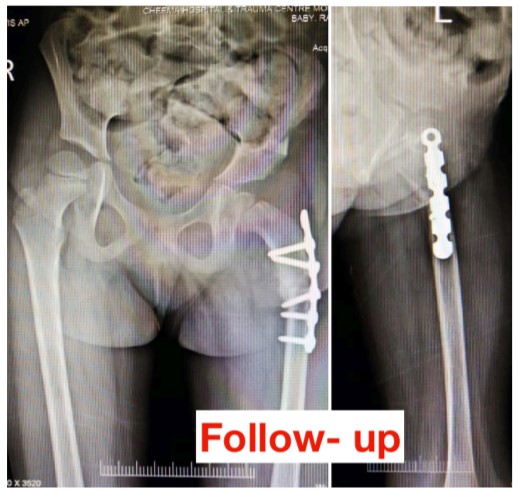

Here comes the Good News! She now walks with a normal gait. She can run without any limp. The subtle residual shortening is expected to be compensated naturally over next few years.