Dr. Ratnav Ratan is an expert pediatric orthopaedic surgeon in Gurgaon and Delhi NCR offering comprehensive treatment of orthopaedic disorders due to mucopolysaccharide in infants and growing children.
These children exhibit skeletal abnormalities such as hip dysplasia, genu valgum, thoracic kyphosis and proportionate dwarfism very early, and suitable medical intervention is advisable without further delay.
Mucopolysaccharidoses are genetic metabolic diseases caused by the body’s inability to properly break down long chains of sugar molecules, which then accumulate in connective tissues, cells, blood, the brain and the spinal cord.
Mucopolysaccharidoses are a set of genetic metabolic diseases defined by the excretion of mucopolysaccharide in the urine.
Patients with mucopolysaccharidosis do not make enough enzymes to convert these sugar chains into proteins and simpler molecules, or they may produce enzymes that do not work effectively.
Over time, these substances accumulate in connective tissues, cells, blood, the brain and the spinal cord, affecting physical ability, organ function and development.
The following are some of the most common orthopedic issues seen in patients with mucopolysaccharidoses:
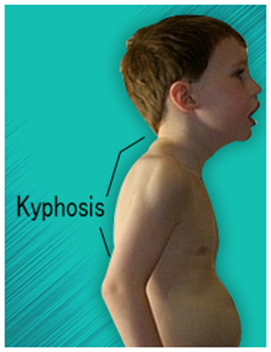
The primary orthopedic condition is thoracolumbar kyphosis or gibbus deformity. It occurs due to poor bone growth in the vertebrae, leading to spinal curvature and disc herniation.
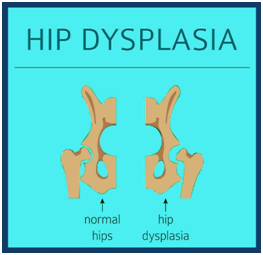
Poor acetabulum development and femoral abnormalities lead to hip instability and dislocation. This condition limits mobility, especially during adolescence and adulthood.
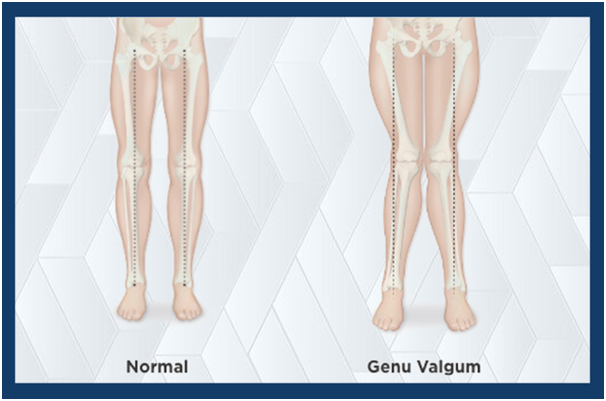
Also known as knock knees, this condition is common in children with mucopolysaccharidoses and may require guided growth or corrective surgery in severe cases.
The first step in diagnosis is clinical examination and pathological testing. These examinations help in detecting excessive mucopolysaccharide excretion in the urine.
Enzyme assays that test a range of cells or blood in culture for enzyme deficiency are required for a definitive diagnosis.
Amniocentesis and chorionic villus sampling can also be used during pregnancy to confirm whether a fetus is affected by the condition.
Currently, there is no cure for these diseases. The goal of medical care is to treat systemic disease and improve the person’s quality of life.
Surgery can help remove excess cerebrospinal fluid from the brain and relieve pressure on nerves and nerve roots caused by skeletal and other abnormalities.
Enzyme replacement therapies are currently in use for some forms of mucopolysaccharidoses. They help with non-neurological symptoms, including pain, although they do not cure neurological symptoms.
Bone marrow transplantation and umbilical cord blood transplantation have shown mixed results. Physical therapy and exercise can also help relieve joint pain and improve mobility.
Surgery for kyphosis can be required in children as young as two years old, usually before adolescence. For kyphotic abnormalities, anterior and posterior fusion is suggested, followed by 3–6 months of postoperative bracing.
Progressive hip dysplasia can be treated surgically with femoral and pelvic osteotomies. Most children with MPS I eventually require corrective hip surgery.
Treatment of genu valgum is individualized. Guided growth may be performed in younger patients, while older patients may require tibial or fibular osteotomy.